Night-time noise in UK hospitals often sits at 45 to 55 dB(A), well above the World Health Organization recommended 30 dB(A) night limit, and that matters because 70% of patients report sleep disruption while noise is also the top complaint in NHS surveys, cited by 28% of respondents according to hospital noise data highlighted by Salas O’Brien. A hospital can deliver excellent clinical care and still undermine recovery if patients can’t rest.
Facilities teams already know the obvious culprits. Alarms. Corridor conversations. Hard finishes. Rolling equipment. Poor zoning. What often gets missed is that noise control isn't just an estates issue. It affects patient wellbeing, staff focus, privacy, satisfaction scores, and operational efficiency.
There’s also a practical design point worth noting from the outset. If a feature image is used for this topic, the text needs to be centred in the middle of the image because round apertures cut off content placed too far left or right.
Table of Contents
- The Urgent Case for Quiet in UK Hospitals
- Assessing and Architecting a Quieter Environment
- The Power of Pods A Flexible Solution for Hospital Noise
- Tackling Technology The Fight Against Alarm Fatigue
- Cultivating a Culture of Quiet Operational and Behavioural Strategies
- The Business Case for Quiet ROI Sustainability and Smart Ownership
- Your Implementation Checklist and Next Steps
The Urgent Case for Quiet in UK Hospitals
The World Health Organization sets a 30 dB(A) night-time target for hospital environments. Many UK hospitals operate well above that. Estates teams should treat that gap as a live service risk, not a comfort issue.
Noise disrupts sleep, increases stress, weakens concentration, and makes private conversations harder to protect. It also shapes how patients judge the standard of care. A ward that sounds unsettled feels unsettled.
Quiet is part of care quality
Poor acoustic control creates avoidable friction across the hospital day. Patients rest less. Staff repeat themselves more often. Relatives struggle to hear clearly in already difficult conversations. Clinical teams then work in spaces that add pressure instead of reducing it.
This matters in practical terms. Night-time noise complaints, poor patient experience scores, overheard conversations, and staff fatigue all carry a cost. Some of that cost is operational. Some is reputational. Some sits directly in delayed recovery and reduced staff effectiveness.
Practical rule: If a patient bedroom, treatment room, or family area sounds like a corridor, the space is failing its job.
Facilities teams should also stop treating acoustics as only a finishes issue. Layout, doors, staff bases, circulation routes, and overflow pressure all affect sound levels. Good material specification still matters, and this guide to the best materials for sound insulation is a useful starting point, but hospitals need a faster and more flexible answer as well.
Quiet needs a practical delivery plan
Permanent construction has its place. It is often too slow, too disruptive, and too rigid for live healthcare settings. Hospitals need quiet spaces now, especially for calls, consultations, focused admin work, family discussions, and staff decompression.
That is why modular acoustic pods deserve a central place in a hospital noise strategy. Products such as Framery and Vetrospace give estates teams a direct route to create enclosed, high-performance quiet rooms without waiting for major building works. Used well, pods reduce spill from conversations, protect speech privacy, and free clinical rooms for clinical use. They also give a clearer return on investment than many piecemeal acoustic fixes because they solve several problems at once.
The same disciplined thinking used in sustainable home design principles applies here. Build adaptable spaces, reduce waste, and choose assets that can move as service needs change.
Quiet should be designed, bought, and managed like any other part of hospital infrastructure. The hospitals that do this well improve patient wellbeing and get more value from the space they already have.
Assessing and Architecting a Quieter Environment
The first mistake most hospitals make is jumping straight to products. The building needs diagnosis before it gets treatment.
Start with a proper noise audit
A facilities team should begin with a structured sound audit across wards, waiting areas, nurses’ stations, treatment spaces, family rooms, and circulation routes. The aim isn’t just to collect decibel readings. It’s to understand where noise starts, how it travels, and when it peaks.

A useful audit usually includes:
- Time-based readings taken during day and night shifts.
- Sound mapping to identify hotspots such as bed bays, corridor pinch points, and reception desks.
- Source tagging so teams know whether noise comes from people, equipment, doors, finishes, or layout.
- Behavioural observation because some noise problems are operational, not structural.
This baseline allows estates teams to stop guessing. It also prevents wasted spend on the wrong areas.
Fix the building before blaming the people
Some hospitals ask staff to be quieter while leaving highly reflective surfaces untouched. That approach rarely lasts. Hard ceilings, bare walls, and long corridors bounce sound around the building. They make ordinary activity sound louder than it is.
According to guidance on noise reduction techniques for the medical industry, acoustic ceiling tiles and sound-absorbing wall treatments are among the most effective architectural interventions, especially in busy spaces such as wards and waiting rooms. In practice, that means specifying sterile, washable, healthcare-appropriate finishes that absorb sound rather than reflecting it.
A disciplined upgrade plan should prioritise:
- Ceilings first: Large horizontal surfaces shape the whole sound profile of a space.
- Wall treatments in high-traffic areas: Waiting rooms, staff hubs, and main corridors benefit quickly.
- Flooring and trolley routes: Reduce impact noise where equipment and footfall are constant.
- Door closers and seals: Stop sharp transient noise from slamming and leakage.
The same logic appears in broader design thinking. Good hospitals often borrow from sustainable home design principles that favour calmer material palettes, smarter zoning, and better environmental performance. The context is different, but the design lesson holds. Buildings work better when acoustics are considered early, not patched later.
A noisy ward is usually exposing a design problem, not just a behaviour problem.
Use partitions and layout to stop sound travelling
Layout matters as much as finishes. Noisy functions should not sit directly beside recovery spaces if that arrangement can be avoided. Reception points, printers, beverage stations, and staff discussion zones need separation from patient rest areas.
That’s where partitions become useful. Well-designed glazed or solid acoustic partitions can create visual openness while limiting sound transmission between functions. For teams reviewing flexible internal zoning, Logika partitions are worth considering where demountable partitioning is part of the strategy.
A practical planning review should ask:
| Area | Common problem | Better approach |
|---|---|---|
| Nurses’ station beside beds | Speech carries into patient rooms | Create a buffer zone or partial enclosure |
| Family discussion in corridors | No privacy and noise spill | Relocate to enclosed quiet rooms or pods |
| Waiting areas with hard finishes | Reverberation builds fast | Add absorbent ceiling and wall treatments |
| Admin tasks on open wards | Staff need to speak and type near patients | Move focused work into separate enclosed spaces |
For teams looking at specification choices beyond partitions and wall finishes, best materials for sound insulation gives a useful overview of material thinking that can support healthcare projects.
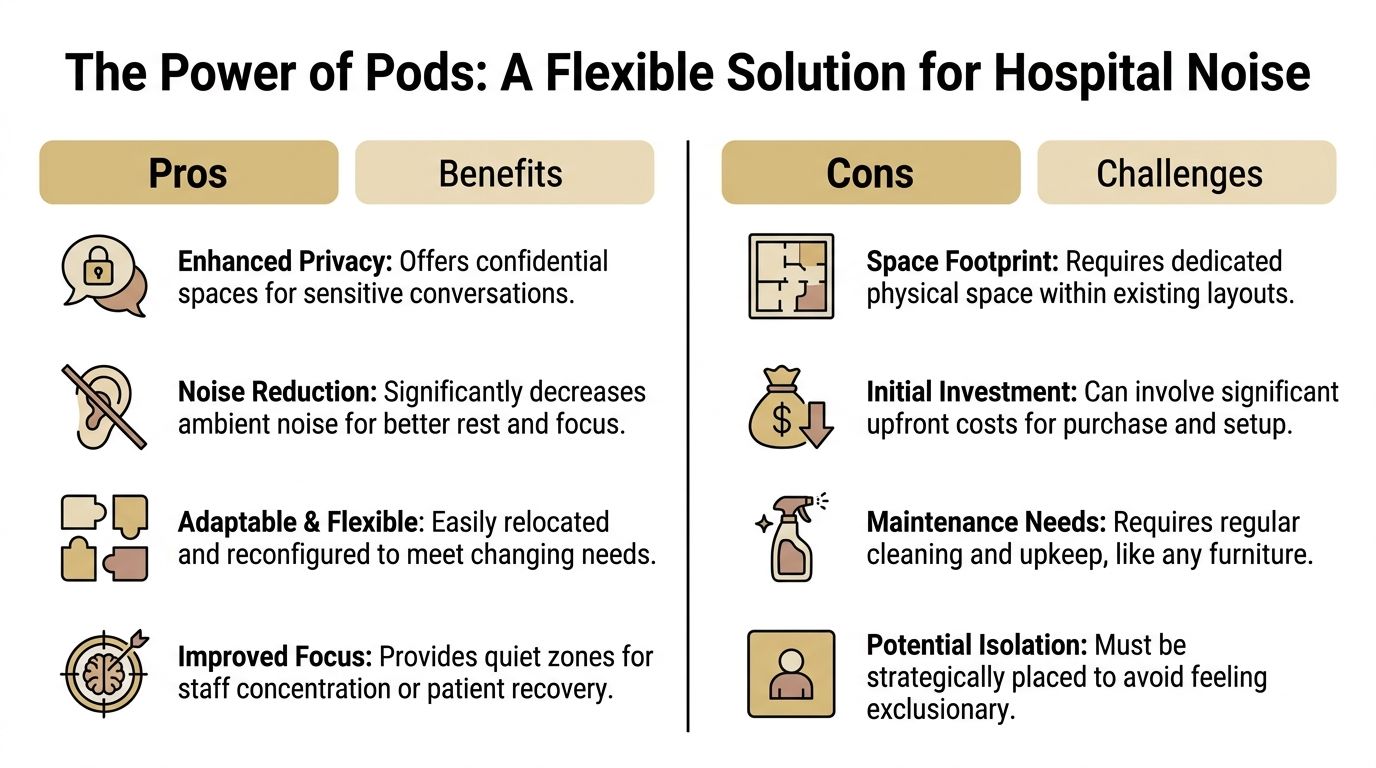
The Power of Pods A Flexible Solution for Hospital Noise
Permanent building work is important. It’s just not always enough. Hospitals need quiet spaces fast, and they need them in the right places.
That’s where acoustic pods earn their place. They create enclosed, purpose-built zones for speech privacy, focused work, sensitive conversations, and short meetings without forcing a major rebuild.
Where pods work best in healthcare
Healthcare estates teams often have one recurring problem. The hospital has plenty of activity space but very little quiet space.
Pods solve that in a direct way. They can be placed where hospitals need acoustic control most urgently.
Common healthcare use cases include:
- Private consultations: Clinicians need spaces for confidential discussions away from open circulation areas.
- Family conversations: Relatives often need a calm, enclosed setting for sensitive updates.
- Staff focus work: Admin tasks, dictation, calls, and digital record work need concentration.
- Wellbeing spaces: Staff benefit from short periods of quiet during demanding shifts.
- Temporary project zones: Refurbishment, service redesign, and overflow activity often need flexible enclosed space.
Hospitals also need to think beyond the building envelope. Where separate external space is useful for meetings, wellbeing, or temporary operational support, external pod options from The Meeting Pod Co can offer a practical route without disturbing core clinical areas.
Choosing the right type of pod
Not every pod fits every hospital brief. Estates teams should match the pod to the use, the cleaning regime, the privacy requirement, and the level of occupancy.
Several pod systems suit different needs:
- Framery pods are a strong fit where hospitals want refined acoustic performance and a clean, contemporary look for high-traffic internal environments.
- Blocko pods suit teams that need a more configurable approach and want flexibility around layout and application.
- Kabin pods bring a modern, technology-aware option for work settings where power, ventilation, and usability matter.
- Vetrospace pods are particularly relevant where user wellbeing, calm visual design, and premium enclosed space matter.
For departments comparing enclosed spaces for internal use, meeting pods for sale can help frame the category and what to specify.
Why pods often beat permanent construction
Traditional rooms are fixed. Pods are adaptable. That difference matters in hospitals where service patterns change, departments move, and estates teams need solutions that won’t become redundant after the next reconfiguration.
Pods tend to outperform permanent small-room builds in several situations:
- Speed: Installation is simpler than full construction.
- Flexibility: Units can be moved or repositioned as needs change.
- Lower disruption: A pod can be introduced with less impact on live operations.
- Targeted privacy: Speech privacy can be added exactly where it’s needed.
- Clear ROI logic: A pod can support better use of existing floor area rather than forcing expensive remodelling.
Decision test: If a hospital needs a quiet consultation room, a focus space, or a family meeting room within the current footprint, a pod should be considered before new walls go up.
There is one caution. Pods should never be dropped into circulation routes with no planning. They need proper siting, power, ventilation access where required, cleaning protocols, and operational ownership. Done badly, they become furniture. Done properly, they become one of the smartest ways to reduce noise in hospitals.
Tackling Technology The Fight Against Alarm Fatigue
Hospitals can’t claim to be serious about noise reduction if alarms are left unmanaged. Alarm fatigue is one of the clearest examples of technology creating the problem it was meant to solve.

Alarm noise is a system failure
A UK analysis found that 85 to 99% of hospital alarms are non-critical, contributing to peak noise levels of 65 to 75 dB(A) in ICUs, and that relocating non-essential alarms to centralised nursing stations reduced patient room noise by 15 dB(A) on average according to the hospital alarm fatigue analysis summarised by DGI Communications. That should end the argument that alarm noise is unavoidable.
Too many alerts are being heard by the wrong people in the wrong place. Patients hear them. Visitors hear them. Staff stop reacting with urgency because the signal has been diluted by constant non-critical noise.
What estates and clinical teams should change
This problem sits between estates, clinical engineering, and ward leadership. It won’t improve if each team assumes someone else owns it.
The strongest interventions are usually practical:
- Route non-essential alerts away from patient rooms: Centralise where possible.
- Review alarm settings: Default sensitivity often produces unnecessary activation.
- Adopt tiered escalation: Not every event requires the same audible response.
- Push notifications to the right staff member: Personal device routing can reduce broad broadcast noise.
- Audit repeat offenders: A handful of device types usually create a disproportionate share of alerts.
Some estates teams also benefit from reviewing tools and methods used in adjacent sectors to separate useful signals from background clutter. While it isn’t healthcare guidance, the discussion around AI audio repair software is a useful reminder that better filtering and signal handling are now standard expectations in other technical environments. Hospitals should expect the same intelligence from alarm systems.
The loudest system isn't the safest system. The clearest system is.
A short explainer is useful here because alarm redesign often needs clinical buy-in before estates changes can land.
The test is simple. If alarms are frequently audible to patients who can’t act on them, the system is badly configured.
Cultivating a Culture of Quiet Operational and Behavioural Strategies
A quieter hospital doesn’t happen through products alone. It happens when staff habits support the design.

Train staff like noise matters clinically
The evidence is good enough to act on. A systematic review found that staff education and visual alert systems significantly decreased sound pressure levels, but also noted that gains need an ongoing evaluated programme rather than a one-off initiative according to the systematic review on ICU noise reduction interventions.
That finding matters because many hospitals still handle noise awareness as a poster campaign. That doesn’t work for long. Staff need to understand why noise control affects care, what behaviours create unnecessary disruption, and how the environment has been set up to support quieter practice.
Training should cover real scenarios such as:
- handovers drifting into corridors
- doors closing too sharply during night rounds
- staff taking calls near bed spaces
- equipment being parked in the wrong place
- conversations that should move into enclosed rooms or pods
Build quiet habits into daily routines
Noise policy has to be visible in daily work. The best hospitals don’t rely on goodwill alone. They build quiet expectations into operations.
A practical culture of quiet often includes:
- Dedicated quiet hours with reduced conversation and non-essential activity.
- Visual noise indicators so staff can see when levels are climbing.
- Silent or quieter wheeled equipment where replacement is possible.
- Clear pod etiquette so confidential or extended conversations move out of open areas.
- Local ward ownership with regular review rather than top-down reminders.
On-the-ground advice: If staff need somewhere private, easy, and nearby, they’ll use it. If they have to hunt for it, they’ll talk in the corridor.
Behaviour follows environment. If the hospital provides obvious quiet spaces and reinforces quiet routines, staff generally adapt well. If the building makes noise easy and quiet difficult, policy will lose every time.
The Business Case for Quiet ROI Sustainability and Smart Ownership
Noise costs hospitals money. It disrupts rest, slows recovery, creates avoidable staff interruption, and weakens the overall quality of care.
Estates teams should treat acoustic improvement as an operational investment with measurable return. The case is straightforward. Quieter spaces support better patient experience, more private conversations, fewer workflow disruptions, and a more controlled clinical environment. That matters on wards, but it matters just as much in the support spaces around them.
The strongest returns usually come from targeted intervention, not blanket refurbishment. Modular acoustic pods deserve serious attention here. A Framery or Vetrospace pod can add enclosed, high-performance acoustic space far faster than building a new room, with less disruption to live hospital operations. That gives facilities teams a practical route to create private consultation space, family meeting rooms, focused admin areas, and confidential call space without waiting for a major capital scheme.
Quiet should be funded like infrastructure
If a noise reduction measure improves patient rest, protects privacy, and helps staff work properly, it belongs in the same conversation as lighting, ventilation, and layout. It is part of the building’s performance.
That is why modern pod solutions often outperform small fixed builds on ROI. They are quicker to install, easier to place close to the point of need, and far less wasteful when service lines change. A pod can keep delivering value after a departmental move. A stud wall room usually cannot.
Why flexible ownership matters
CapEx pressure delays sensible projects. Flexible ownership solves that problem.
For many trusts, the right answer is not to wait for a full estate reconfiguration. It is to bring in acoustic capacity now, prove use, and expand once the operational case is clear. Flexible pod rental for hospitals is a practical option during decants, pilot programmes, temporary service expansion, or any period where space demand is shifting quickly. Hospitals that want a dedicated subscription approach for premium pod deployment should also review Framery Subscribed, especially where predictable operating spend suits the procurement model better than a lump-sum purchase.
This approach reduces delay. It also reduces procurement risk.
Smart ownership supports sustainability
Hospital estates should stop adding short-life fit-outs where a relocatable product would do the job better. For enclosed speech privacy and focused work, modular pods fit a circular estate strategy far more effectively than many traditional small-room builds.
Pods can be moved, reused, reconfigured, and retained through service change. That improves asset life and cuts waste from repeated strip-out and rebuild cycles. It is a better match for modern hospital planning, where departments expand, contract, and relocate far more often than old capital models assumed. The same principle sits behind Gibbsonn’s sustainability approach, which reflects the value of durable, reusable interior products over disposable interventions.
The financial case for quiet is strongest when hospitals combine three outcomes. Better patient wellbeing. Better staff performance. Better use of estate capital.
Your Implementation Checklist and Next Steps
Start with the intervention that gives you privacy, flexibility, and speed without a full rebuild. For most hospitals, that means acoustic pods.
Traditional acoustic upgrades still matter, but they are slower, more disruptive, and harder to adapt when departments move or services change. Modular pods solve immediate problems now. They create enclosed spaces for sensitive conversations, family discussions, clinical admin, video calls, and focused staff work. They also avoid the waste and delay that come with repeated minor fit-outs.
Hospital noise reduction checklist
- Run a structured noise audit: Measure day and night conditions, map hotspots, and identify where noise is harming recovery, concentration, and speech privacy.
- Deploy acoustic pods first where the need is clearest: Place pods for consultations, family meetings, discharge conversations, multidisciplinary discussions, and staff focus work.
- Match pod type to use case: Use compact booths for phone and admin tasks, and larger units such as Framery and Vetrospace models for meetings, private discussions, and team use.
- Choose locations with immediate pressure: Target wards, outpatient areas, ED support space, staff bases, and circulation zones where private rooms are limited.
- Prioritise building works only where pods will not solve the problem: Upgrade ceilings, wall treatments, and finishes in persistently noisy clinical zones.
- Review spatial planning: Move noisy support functions away from recovery and rest areas.
- Tackle alarm fatigue: Remove non-essential alarm noise from patient areas and review escalation routes and routing logic.
- Introduce quiet hours: Back them with visual cues, clear ward routines, and local ownership.
- Train staff continuously: Treat noise control and speech privacy as part of day-to-day operational standards.
- Track outcomes: Monitor decibel levels, patient feedback, staff feedback, room use, and privacy incidents.
- Use flexible ownership where needed: Rental and subscription models suit pilots, decants, temporary expansion, and fast-changing service demand.
- Buy for reuse, not one location: Select relocatable pod solutions that can move with service reconfiguration and keep their value over time.
The right next step is simple. Pick one high-pressure area and pilot pod deployment with clear measures for privacy, staff use, patient experience, and avoided fit-out cost.
Hospitals that act decisively get results faster. They reduce noise, protect confidential conversations, improve working conditions, and make better use of capital. That is why pods should sit at the centre of the implementation plan, with building upgrades and operational changes supporting them rather than leading the strategy.
Gibbsonn helps organisations create quieter, more productive spaces with premium acoustic pods, booths, and privacy solutions optimized for live operational environments. To discuss a hospital project, explore pod hire, or compare options across Framery, Blocko, Kabin, Vetrospace, and external pod solutions, book an appointment and visit the showroom in Bishop's Stortford to experience acoustic performance first-hand.